An 80 year-old woman presented to the ED with a chief complaint of ‘constipation’. Constipation is a missed diagnosis waiting to happen. It’s extremely difficult to justify not obtaining some type of imaging study. And those with constipation nearly always warrant a digital rectal exam.
In an unrelated case that went to peer review, an elderly male came in for constipation. The ED physician ordered an x-ray which showed…constipation. She advised the person to use over-the-counter Miralax and discharged them home. The person returned 12 hours later with a bowel perforation. The surgeon’s issue with the ED care was that a rectal exam was not performed, so a fecal impaction could not be ruled out. Furthermore, the patient was advised to take oral medications to alleviate the constipation – this might have worsened the obstruction and portended a perforation. It didn’t end well for the ED physician.
Back to our case: an x-ray was done and there was some concern about some badness so a CT scan was ordered. Here are the images:
If for some reason the video will not play, here is a still shot:
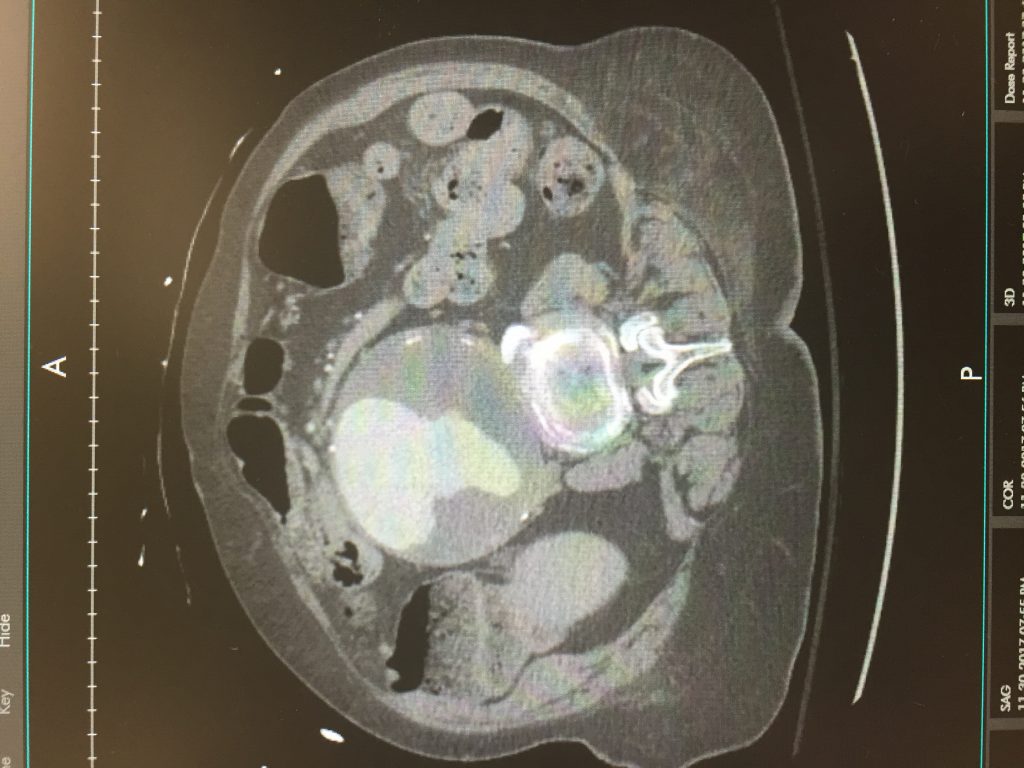
Official measurements of the aneurysm are 9.4 x 9.6cm beginning at the level of the renal arteries. The patient was started on an esmolol drip and admitted to the vascular surgeon.
Abdominal Aortic Aneurysms:
Aneurysm repair is the primary treatment for aneurysms that are symptomatic or at a high risk for rupture. Elective surgical repair should be considered for aneurysms > 5.0–5.5 cm.
Ruptured abdominal aortic aneurysms have a near 100% mortality rate without immediate operative repair.
The annual risk of rupture based upon aneurysm size is estimated as:
- < 4.0 cm in diameter = less than 1 in 200
- 4.0 to 4.9 cm in diameter = between 1 in 200 and 1 in 20
- 5.0 to 5.9 cm in diameter = between 1 in 30 and 1 in 7
- 6.0 to 6.9 cm in diameter = between 1 in 10 and 2 in 10
- 7.0 to 7.9 cm in diameter = between 2 in 10 and 4 in 10
- 8.0 cm or more in diameter = between 3 in 10 and 5 in 10
Smoking cessation is the only known way of decreasing aneurysm enlargement.



{kind=link}