
Working in the ER has been compared to walking through a minefield in clown shoes. Stepping on a mine is inevitable; you rely on sound decision-making and a good patient/doctor relationship to minimize the ‘blast’.
We are hit with a lot of interruptions on each shift, not the least of which is a steady barrage of EKGs to sign. It is imperative to take a close look as one signature from you may mean deflecting the patient to the waiting room where they will end up for sitting un-monitored.
Here is an EKG I was hypothetically handed on a recent shift. I was given the EKG along with the triage nurse’s clinical opinion: “he has some non-specific pain in his upper abdomen and looks fine.”
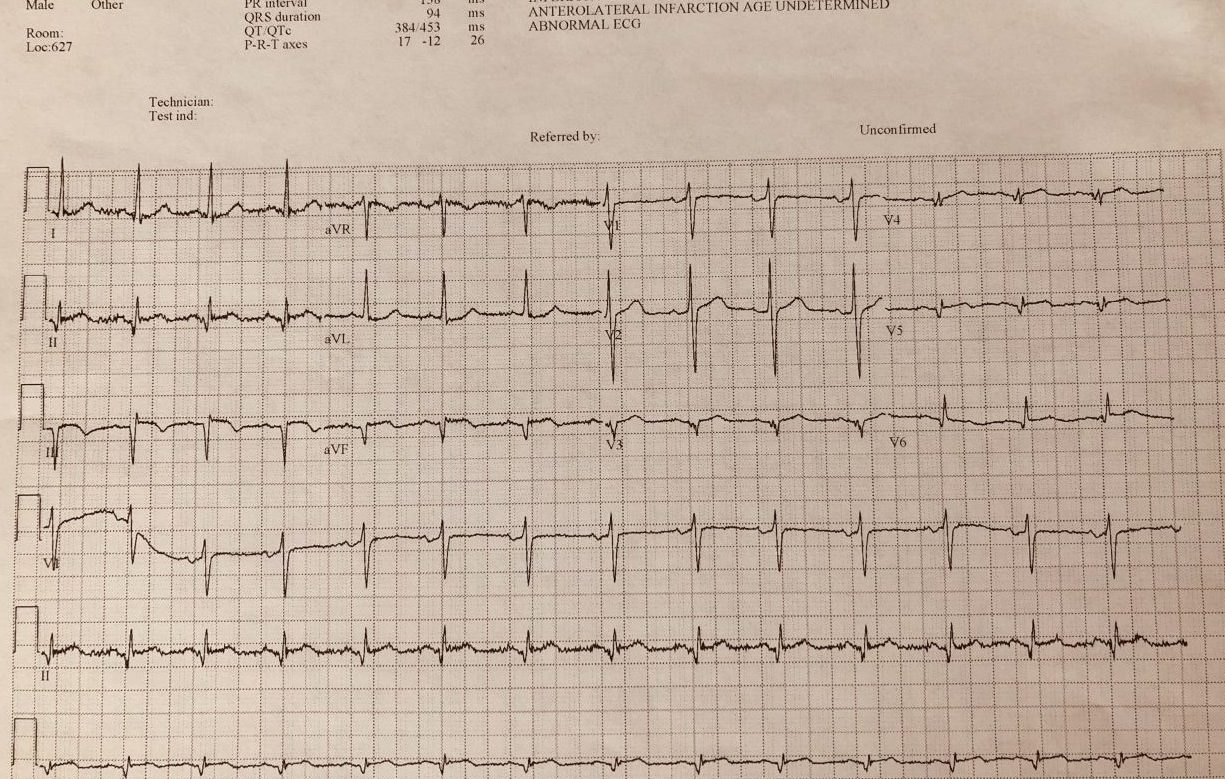
I think lead III is fairly obvious but the others are much more subtle. A ‘STEMI’ was activated, and sure enough, the patient had a very atypical story. Bilateral lower chest ache for three days. No medical history. Looked fine. I asked for a repeat EKG and here is one from five minutes later:
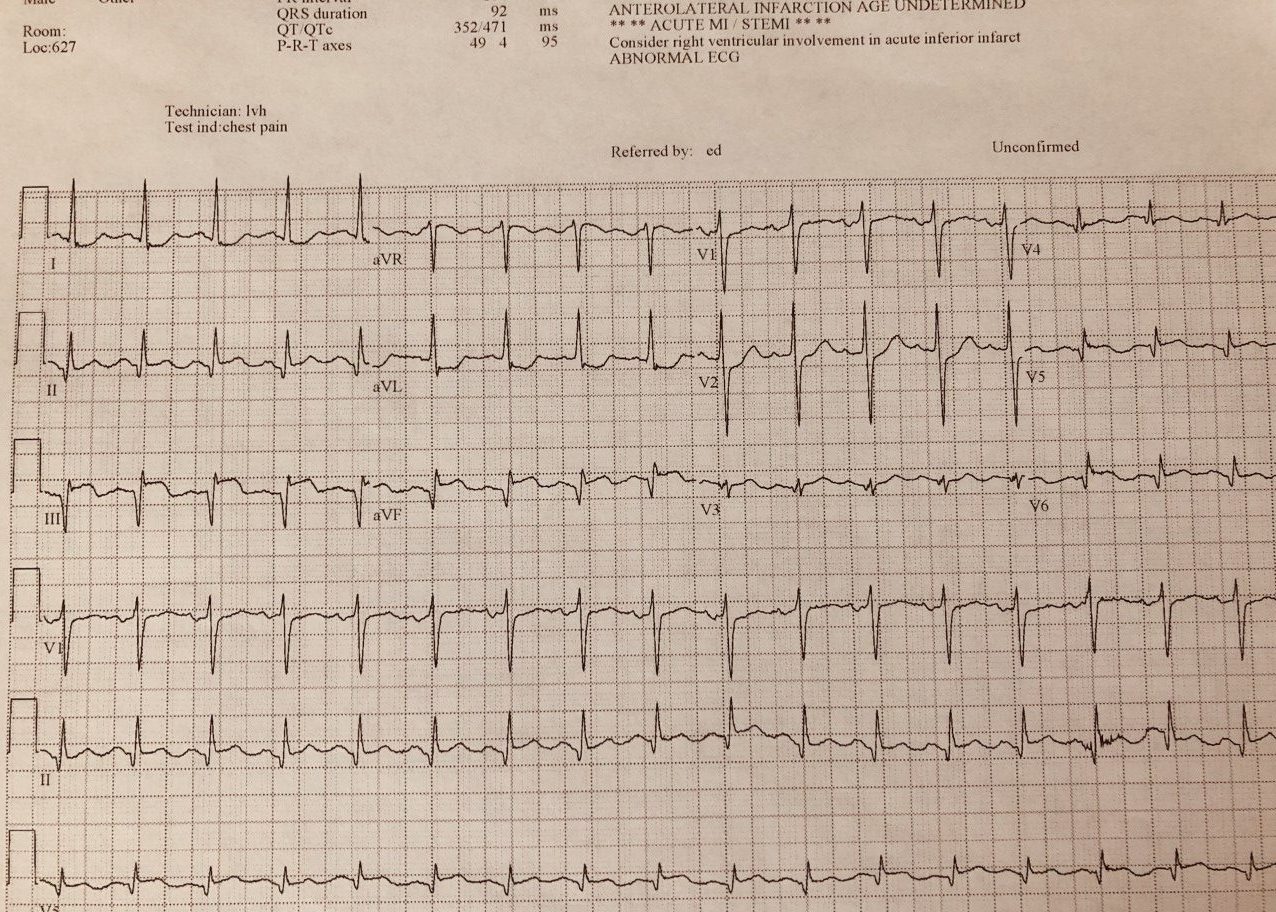
The patient was taken to the cath lab where a near complete RCA lesion and a 100% LAD occlusion were identified.
Take-home points:
1. Review all EKGs closely. This is your first opportunity to evaluate for the presence of an emergency. Most times, you don’t have the patient in front of you and haven’t even spoken to them yet.
2. The machine’s interpretation can sometimes help remind you to look for something, but never rely on that. You can see from above that the machine did not identify the ST elevation on the first EKG.
3. Don’t let the nurse report distract you. I can’t even count the number of times ancillary staff has downplayed a patient’s complaint or presentation only for me to find real pathology. Don’t let others’ opinions bias you.
4. Good luck with #3.



{kind=link}