All antibiotics come with side effects. Some are fairly innocuous, like an upset tummy. Others are a little more serious, like aortic dissection and death. The beauty of medicine is that we have more treatment choices now than ever before. And as our antibiotic options expand, we should be willing to let go of dogma and evolve with the times. Case in point: fluoroquinolones.
Fluoroquinolone antibiotics (ciprofloxacin, levofloxacin, moxifloxacin, among others) are an important class of antibiotics that have a specific role. Until fairly recently, ciprofloxacin was a primary treatment option for cystitis. It has been used routinely for inpatient treatment of pneumonia, and many still consider it part of the first-line treatment for diverticulitis. However, in the past few years, concerns regarding its safety profile have multiplied exponentially, and there are few times that it should be used as a first-line treatment.
Some background:
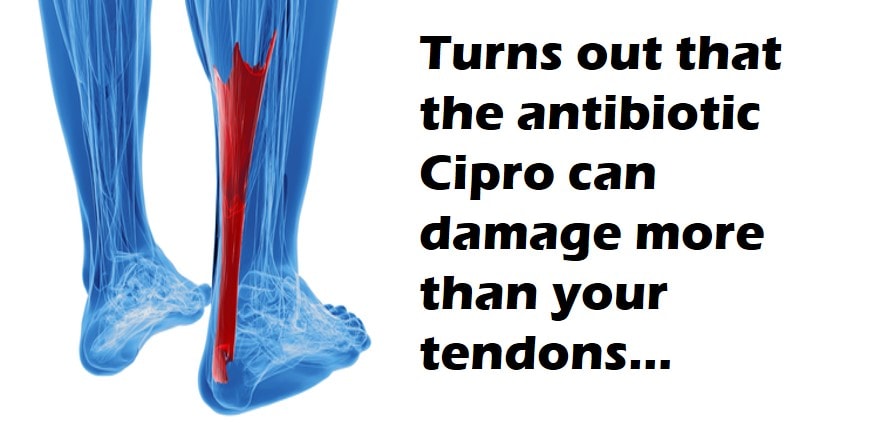
In 2008, the FDA added its first black box warning to fluoroquinolones, indicating the risk for tendon injuries. Despite this, in 2010, levofloxacin was the best-selling antibiotic in the U.S., with sales exceeding $1.5 billion. By 2012, it was the subject of more than 3,000 lawsuits following severe reactions.
The first successful lawsuit involved an 82-year-old male who was prescribed levofloxacin and a corticosteroid for an upper respiratory infection. He suffered bilateral Achilles tendon ruptures and was ultimately awarded $1.8 million. In a large population-based case control analysis, patients treated with fluoroquinolones had a 4x increase in risk of Achilles tendon rupture and a 46x greater risk if there was concomitant use of corticosteroids.
Symptoms of tendinopathy typically begin about 6 days after the onset of treatment, but the risk of tendon rupture persists for up to 90 days.
Okay, so it can cause ruptured tendons. What else?
A 2012 study published in JAMA found that oral fluoroquinolones were associated with an increased risk of developing retinal detachment. Current users of oral fluoroquinolones were nearly 5x more likely to be diagnosed with retinal detachment than non-users.
Eyes, tendons, is there more???
Another case-control study attempted to quantify the risk of acute kidney injury. Researchers found a 2x higher risk of acute kidney injury in patients taking fluoroquinolones.
Great, anything else I need to know before I stop prescribing this dangerous drug?
This is where it gets interesting…
A study in JAMA Surgery found that patients who received fluoroquinolones had a higher risk for aneurysms, ruptures, or dissections than those who did not receive the antibiotics. The study showed that normal, unstressed mice who took the antibiotic did not show significant negative effects on the aorta. Mice with moderately stressed aortas who were given fluoroquinolones developed aortic aneurysm and dissection 79% of the time, compared to 45% of those moderately stressed mice who did not receive the antibiotic. This led the FDA to issue the following statement in December 2018:
“A U.S. Food and Drug Administration (FDA) review found that fluoroquinolone antibiotics can increase the occurrence of rare but serious events of ruptures or tears in the main artery of the body, called the aorta….Fluoroquinolones should not be used in patients at increased risk unless there are no other treatment options available. People at increased risk include those with…high blood pressure, certain genetic disorders that involve blood vessel changes, and the elderly…”
There is really only one condition for which fluoroquinolones are still considered first-line treatment:
Inhalational anthrax
If you’re not concerned about inhalational anthrax, consider a different antibiotic.
For years, the go-to outpatient treatment for patients diagnosed with diverticulitis has been 10 days of ciprofloxacin and metronidazole. An acceptable alternative is amoxicillin/clavulanate 875 mg every 8 hours (or 1 g every 12 hours). Trimethoprim/sulfamethoxazole (1 double-strength tablet every 12 hours) can also replace ciprofloxacin and be used in combination with metronidazole.
Summary:
When prescribing fluoroquinolones, consider any reasonable alternative. If there is none, explain the potential risks and benefits to your patient. Document this conversation to minimize risk in the event of a bad outcome.
For a more in-depth discussion, consider this article written by two cool dudes:
https://www.emra.org/emresident/article/fluoroquinolones/
And finally, some food for thought:



{kind=link}