
A male in his 60s presents by EMS with sudden onset of a headache while at work. His initial blood pressure is 210/90mmHg. On exam, he is slow to answer questions and follow commands. He cannot lift either leg off the bed but his exam is otherwise unremarkable. A stat CT head shows:
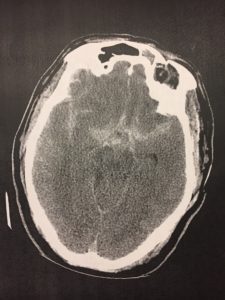

This is a subarachnoid bleed! Classic history for a ruptured aneurysm.
He receives IV antihypertensives and IV keppra, amazingly protects his airway, and is admitted to a neuro-critical care bed for further treatment (coiling/stenting/etc).
How should this patient’s BP be managed?
In cases of spontaneous intracerebral hemorrhage, severe elevations in BP can cause hemorrhage to expand and the patient to further deteriorate. However, maintaining some amount of elevated BP can help maintain CPP.
Remember,
CPP = MAP – ICP
Where CPP is cerebral perfusion pressure, MAP is mean arterial pressure, and ICP is intracranial pressure.
Put another way, if ICP goes up (as it will do if blood is now filling up that space) and MAP goes down, CPP will go down. To maintain CPP, you may need to allow rises in MAP above what you would normally allow.
As per UptoDate, current guidelines for BP management in spontaneous ICH are as follows:
For patients with high BP and no evidence of increased ICP, lower systolic to 160mmHg. However, newer studies have demonstrated that systolic can safely be lowered to 140mmHg.
Labetolol or nicardipine are the agents I most often select.



{kind=link}